


Many practitioners understandably find nasolabial folds (NLF) and dynamic discord lines, a challenge to soften and reinforce with nonsurgical enhancements such as dermal filler or skin boosters. The reasons for this are threefold; a) these areas often look very different on static appearance to dynamic, therefore providing treatment that looks natural in both modalities is a limiting factor, b) the appearance of these lines often comes from both a deep, ingrained rhytid in the dermal layer, as well as shadow from a combination of excess volume and loss of volume in the surrounding fat pads, and c) dermal filler selection for treatment of such lines has been historically challenging as many fillers do not have the rheology to seamlessly blend with the skin on expression. Thus if they are flexible enough to stretch with the skin, they may not be cohesive enough to significantly volumise and vice versa. This may lead to visible lumps or underwhelming results respectively. It would follow that in each case, either the dermal rhytid, the lack or excess of volume, or both should be treated, and that filler selection for the surface rhytid needs flexible yet moderately cohesive rheology, depending on the skin quality.
This paper will demonstrate a novel technique for highly effective treatment of NLFs and dynamic discord lines with dermal filler.
Anatomy of the nasolabial folds
The NLF consists of dermal muscle insertions of risorius, zygomaticus major/minor and levator labii superioris, combined with subdermal fat and tissue of the superficial musculoaponeurotic system (SMAS) (Niamtu, 2019). The SMAS is a complex which can be described as consisting of two parts: type 1 SMAS which is found lateral to the NLF, and type 2 which is found medial to the NLF (Whitney et al., 2023). Type 1 SMAS consists of loose lobules of fat interwoven with fibrous septae. Conversely, type 2 SMAS consists of little fat and therefore is a dense structure tightly adhered to its underlying structures. The different cellular architecture of these SMAS types gives rise to part of the appearance of the topological NLF.
» With age, there is loss of muscular tone in the SMAS, osseous resorption, skin thinning and laxity, fat hypertrophy and descension «
Additionally, there is weakening and laxity in the complex of cheek retaining ligaments which results in further ptosis of malar and nasolabial fat pads, which cannot descend further than the NLF due to strong fascia-dermis connections (Pogrel et al., 1998). The resultant collection of soft tissue superior to the NLF combined with the local anatomical changes, creates the deepening appearance of the NLF we are familiar with.
The NLF may present as a dermal rhytid or shadow cast along the curve from the alar crease to the oral commissure. In many cases there is a combination of these presentations. The NLF may be apparent at rest, however, may appear more severe on smiling. It is important to differentiate whether the NLF complaint in question is due to a dermal rhytid or a shadow, as these are both treated differently.
Anatomy of dynamic discord lines
This term ‘dynamic discord’ refers to the appearance of wrinkles or dermal folds which become pronounced on the function of underlying muscles (Akinbiyi et al.,2020). It is usually a combination of strong muscle action, underlying volume loss and poor-quality overlying skin. The most common facial areas to exhibit this feature are:
- Perioral: radiating from the mouth outwards on contracting orbicularis oris.
- Buccal and lateral cheek: vertical radial cheek lines radiating from the buccal cheek towards the preauricular (van Loghem et al., 2021).
- Periorbital and superiolateral cheek: emanating from the lateral canthus and lower eyelid, discordant lines appear on contracting orbicularis oculi and zygomaticus major/minor.
- Forehead: horizontal lines due to frontalis activation and vertical lines due to glabellar complex contraction.
All of these areas are potential targets for treatment with dermal filler, however these areas vary in their risk of complications such as vascular occlusion, Tyndal l, oedema or lumps. Of note, the glabellar lines are particularly high risk for vascular occlusion with supratrochlear and supraorbital arteries lying just 1.71-3.74mm below the skin surface in the glabellar region (Cotofana et al., 2021). Therefore, caution should be exercised and only experienced and appropriately trained medical injectors should consider treating such areas. Furthermore, where filler treatment is particularly high risk, botulinum toxin treatments should be attempted if appropriate. Likewise the risk of oedema or Tyndall are much higher in the undereye region, and should only be approached with dermal fillers directly by experienced hands, with appropriate assessment of skin laxity, thickness, superficial vessels and lymphatic compromise.
Current non-surgical treatment of the NLFs
Treatment of the NLF should include assessment of the whole face, to identify contributing factors that may be impacting on the appearance of the NLF, such as general skin laxity, loss of lateral cheek volume, laxity of retaining ligaments, hypertrophy and ptosis of nasolabial fat pads, flattened maxilla. If any of these factors are present, addressing them may indirectly improve the appearance of the NLF. Therefore biostimulatory injectable or energy treatments should be employed primarily, followed by restoration of midface volume and volume lateral to the ‘line of ligament’ (Jacobson et al., 2003; Casabonaet al., 2020; Galadari et al., 2015). If the NLF appearance persists, local treatment by bolus deposition in the deep pyriform space with high G’ filler, combined with subcutaneous augmentation with moderate G’ fillers in linear threads and fanning patterns is common. The term G’ represents the elastic modulus of the dermal filler (Faivre et al., 2021). Elastic modulus values indicate how viscous or flexible a material is. The lower the G’ value, the more flexible and fluid it is. A high G’ filler would traditionally be used where more viscous, less elastic filler would be advantageous, such as in the deep supraperiosteal layer. A moderate G’ filler would therefore be somewhat flexible with moderate viscosity and therefore be more suited to mid depth or superficial placement. The deep pyriform and superficial linear thread technique is adequate in restoring overall improved contours and light reflection however may not address a deeply ingrained dermal rhytid.
Novel ‘mini fan’ and ‘simple interrupted thread’ techniques
To address deeply ingrained lines in the NLF or other discordant facial wrinkles, it is important to directly address the dermis, not just the subcutaneous structures. Where the aetiology of these deep lines is repeated folding of the skin, reinforcing and supporting the dermis to provide resistance to folding is key in improving the appearance immediately, as well as preventing future skin damage. A flexible, moderate G’ hyaluronic acid based filler (Teosyal RHA3) can be used to deposit filler in two patterns:
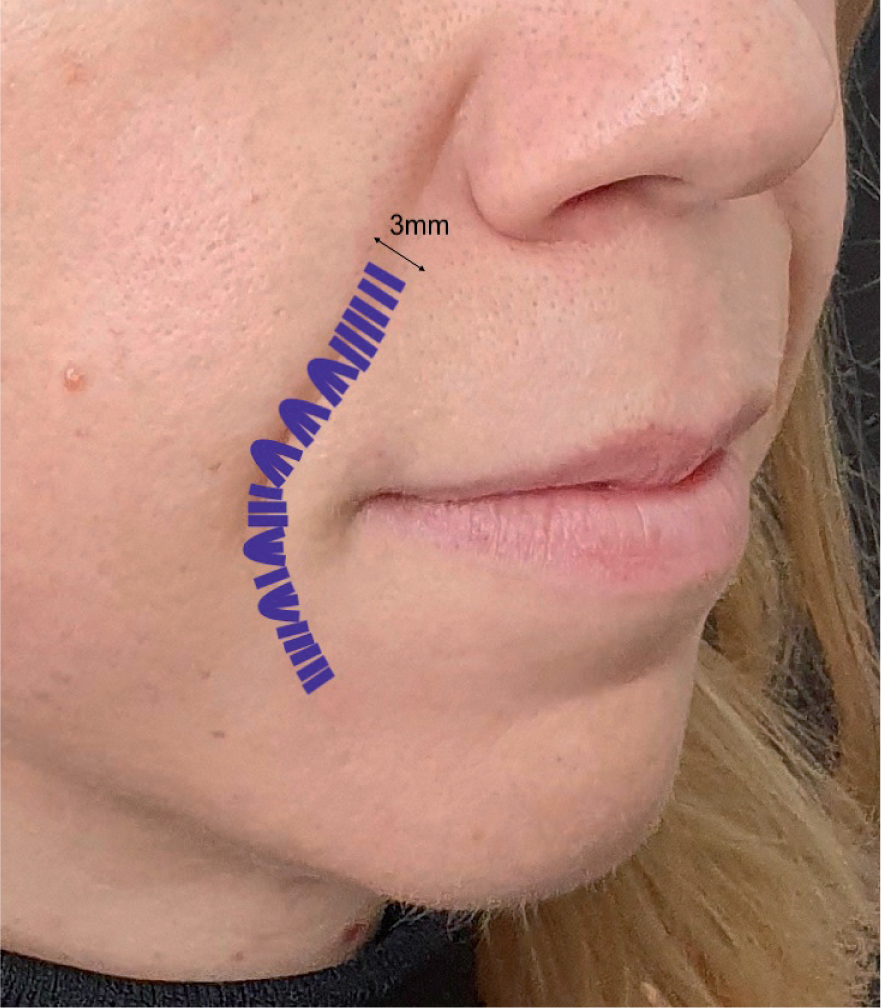
Mini fan
Small fans of filler are deposited intradermally, in a retrograde fashion. The fans bisect the NLF, perpendicular to the course of the rhytid. The entry point is superior to the NLF and the length of each fan is no more than 3mm. These are repeated along the course of the NLF.
Simple interrupted thread
The ‘mini-fan’ technique can be combined with very small retrograde threads intradermally. These are again angled perpendicular to the course of the rhytid and are no more than 3mm in length, with entry points superior to the NLF. The pattern of these threads resembles simple interrupted sutures for primary wound closure.
Inadvertent injection of filler into the nasolabial fat pad is avoided in these techniques, by controlled deposition within the dermal layer, at a shallow needle entry angle. Care is taken not to deposit filler deeper into the subcutaneous superficial fat. It is important this is adhered to as injection into the nasolabial fat pad would worsen the appearance of the NLF. It is also important to maintain the intradermal placement to mitigate the risk of occluding the facial. Safety of the technique is ensured by keeping injections intradermal and therefore superficial to the course of the facial artery and keeping injection volumes low. These techniques require excellent dexterity and control, and therefore only suitable for experienced injectors.
» The mini fan has the benefit of less entry points and therefore enhanced patient comfort. This may be favourable in patients with lower pain thresholds «
Both of these techniques may be used alone or in combination to provide a buttress-like strengthening effect within the dermis itself. The volume of filler used is very low within each mini fan or thread, however, by close juxtaposition, they provide significant resistance to deformation of the NLF skin. The mini fan has the benefit of less entry points and therefore enhanced patient comfort. This may be favourable in patients with lower pain thresholds. The simple interrupted thread has the benefit of being very precise and easier to tightly pack together for the more severe rhytid presentations. The more densely packed together the threads or fans are, the more resistance to deformation and better resolution of the rhytid.
Clinical case
A 31 year old woman presented with concerns about deepening smile lines which she felt were extending to her chin area and not concealable with makeup. On examination she presented with marked midface volume loss resulting in a flat midface profile. She had nasolabial fat pad prominence combined with loss of volume in the pyriform space and a superficial dermal rhytid along the length of the NLF, extending inferior to the oral commissure. To adequately restore the appearance to the lower face, a full-face approach was planned. By treating the whole face rather than purely the lower face, more natural proportions and contours would be achieved and ultimately a more satisfactory final result for the patient. The midface volume would be restored first to improve light reflex along the zygomatic arch and reduce emphasis on the nasolabial fat pad. Then traditional restoration of volume in the pyriform aperture and length of the NLF would be required to reduce shadow and support the skin more effectively. Finally, the novel intradermal injection techniques would give optimal results by strengthening the dermis and providing resistance to rhytid reintroduction.
» By treating the whole face rather than purely the lower face, more natural proportions and contours would be achieved «
The loss of volume in the mid and lower face was addressed first, to help provide maximum subcutaneous support to the rhytids in question. The effect of the traditional approach to NLF treatment can be observed by comparison of Figures 2 and 3. Midface restoration had already been completed in these images. Prior to lower face treatment (Figure 2) the subject had both loss of volume and a deep rhytid along the course of the NLF and inferior to the oral commissures. In Figure 3, traditional treatment shows improvement to the light reflection and very subtle softening of the NLF. This was achieved firstly by deep pyriform bolus deposition with Teosyal Puresense Ultradeep. 0.4ml was deposited to the right side, and 0.3ml to the left. Following this, subcutaneous Teosyal RHA4 was administered in linear threads along the length of the NLF and fanning at the superior portion lateral to ala. 0.5ml was deposited over the right side and 0.3ml to the left, by 38mm 25G microcannula.


Following revolumisation, the novel intradermal mini fan and simple interrupted thread techniques were employed along the full course of the remaining ingrained rhytids. Teosyal RHA3 was used with the proprietary 27G needle. Figure 4 demonstrates the immediate post operative appearance. The novel technique was employed immediately after revolumisation visible in Figure 3. There is clear resolution of the ingrained rhytid appearance bilaterally with an overall more youthful appearance. Despite mild perioperative oedema, there are no lumps or Tyndall effect as the filler selected has good flexibility and was only administered in very small volumes. A total of 0.5ml was used on the right side and 0.8ml used on the left side. All treatment was completed in the same visit. The patient was reviewed at two weeks after treatment to assess resolution of aesthetic concerns. The two week settled post-op results can be directly compared with the pre-op presentation in Figure 5.


Conclusion
NLFs and dynamic discord lines are challenging facial features to adequately treat with dermal fillers. To effectively treat these features, it is important to address their multifactorial aetiology. This means addressing subcutaneous volume loss if present and the dermal rhytid directly. It is important to select appropriate fillers for each indication, with consideration to individual patient's tissue quality, ensuring that a suitably flexible filler is employed for intradermal injection. Traditional treatment of volume loss is effective in reducing shadows however to smooth the appearance of deep dermal rhytids, intradermal ‘mini fans’ and ‘single interrupted threads’ can be administered. These techniques combined can provide impressive resolution of severe NLFs and dynamic discord lines in both static and dynamic appearance.