


In homeostasis, puberty hormones known as androgens (in particular, testosterone) spark a proportion of vellus hairs to transition to terminal hairs (Marieb, 2001). In women, this is characterised by thicker growth in the axilla and genital regions, while, for men, terminal hairs present on the face, chest, back, arms, legs, axilla and genital areas (Marieb, 2001). Homeostatic imbalances upset the status quo between hair loss and replacement and can occur in all phases of human life (Marieb, 2001). Most hair loss diseases and conditions are generally benign and not contagious. Ageing can signal changes in hair growth and, in particular, scalp hair loss (Figures 1 and 2). It has been proven that hair growth and density are regulated by hormones and nutrition (Richards and Merharg, 1995).
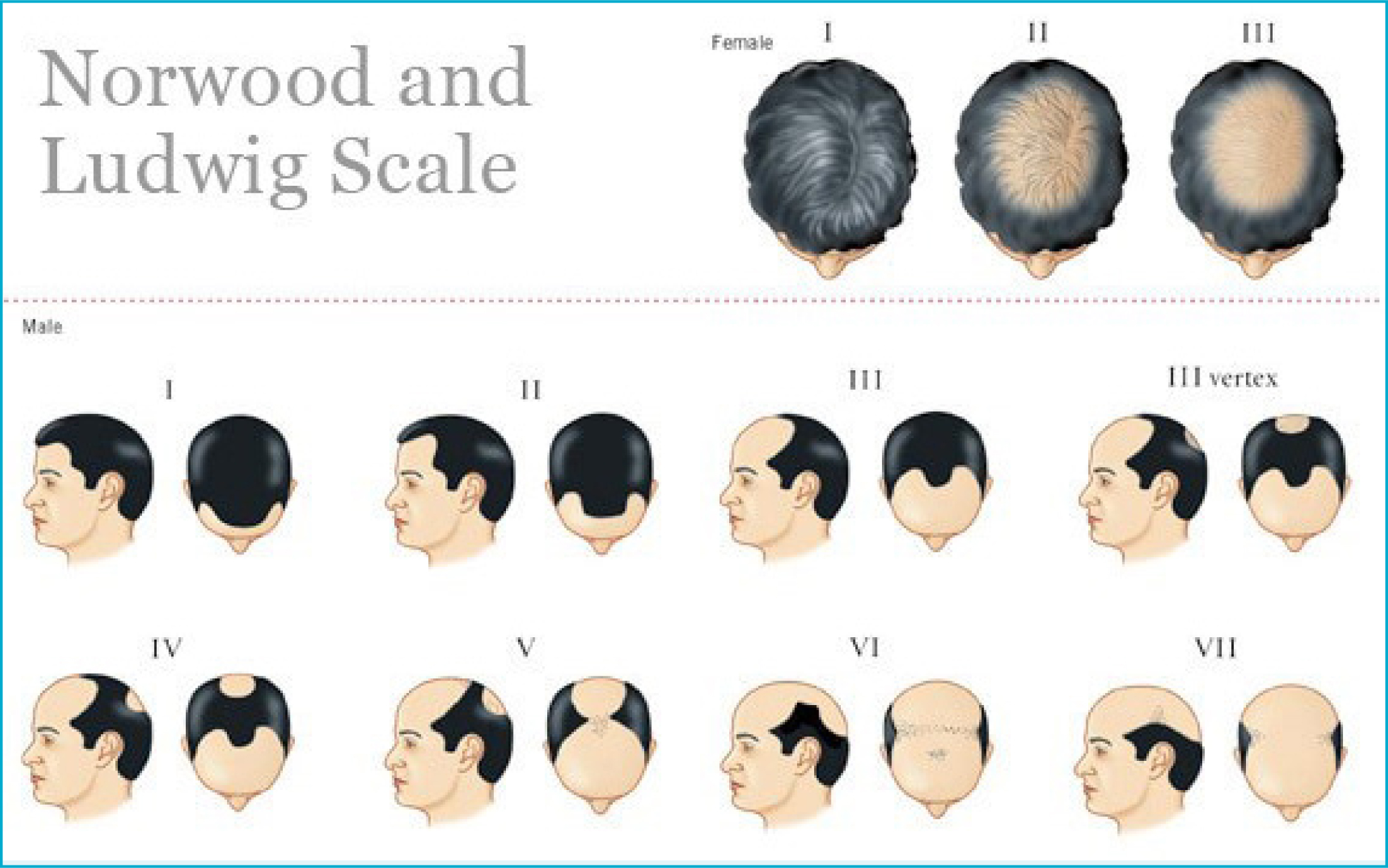 Figure 1. The Norwood-Hamilton scale for male pattern baldness and The Ludwig scale for female pattern hair loss
Figure 1. The Norwood-Hamilton scale for male pattern baldness and The Ludwig scale for female pattern hair loss 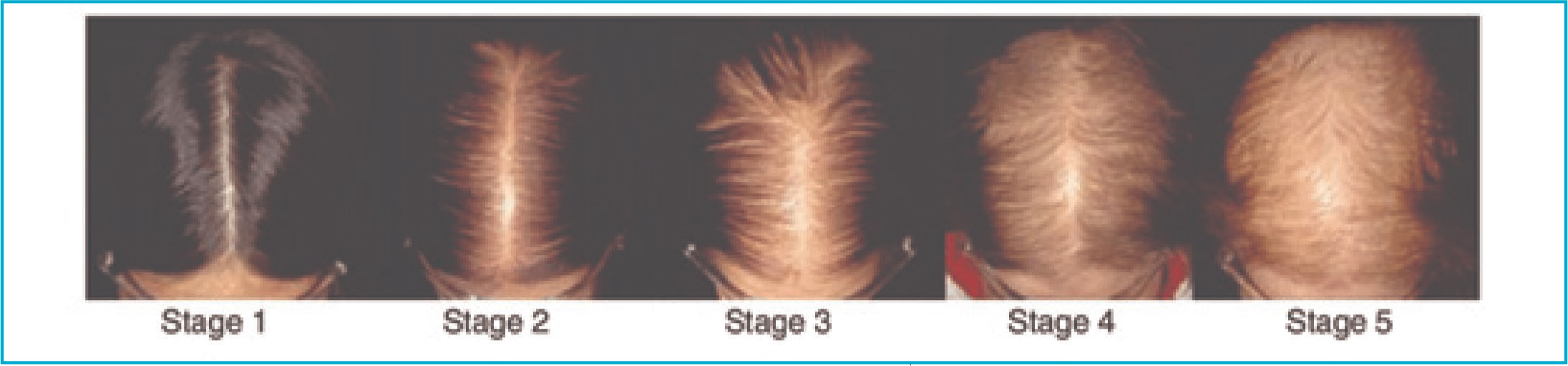 Figure 2. The alternative Sinclair Scale for female hair loss
Figure 2. The alternative Sinclair Scale for female hair loss
With age, hairs are not replaced as fast as they are shed. This leads to hair thinning, which is usually accompanied by some degree of baldness. The medical term for this is androgenetic alopecia, and it can affect both men and women. Androgenetic alopecia (AGA) is a non-scarring (non-cicatricial), benign and chronic condition that is generally related to ageing. Nevertheless, a proportion of the hair can grow back. AGA is also known as male pattern hair loss (MPHL) or female pattern hair loss (FPHL).
Loss of hair is thought to be caused by a delayed action gene that is activated at some point in adulthood and changes the response of hair follicles to testosterone, reversing the growth (Marieb, 2001; Kanti et al, 2018). This genetically inherited sensitivity to the effects of dihydrotestosterone (DHT), the end conversion of testosterone, is regulated by types I and II 5-alpha reductive enzymes (Lee et al, 2018). Features and symptoms of male AGA include the miniaturisation of terminal hairs on the scalp, which become wispy and translucent vellus hairs. The shortening of the anagen hair cycle contributes to this. Shrinkage of the follicle means that it is no longer visible at the surface of the skin (Miron et al, 2019).
Alpha granules contained within platelets are comprised among others of six key growth factors: platelet-derived growth factor (PDGF), insulin-like growth factor-I (IGF-1), transforming growth factor beta (TGF-β), vascular endothelial growth factor (VEGF), fibroblast growth factor (FGF) and epidermal growth factor (EGF). These growth factors, produced in platelet degranulation, upregulate the production of angiogenesis, neocollagenesis and proteoglycans. Crucially, the release of IGF-1 has been shown to promote the anagen phase of hair growth (Gentile and Garcovich, 2020). Key signalling pathways in hair follicle development are mediated through various traffic and the expression of beta-catenin, a genetic marker. Stem cell activity is regulated through cell-to-cell signalling between mesenchyme and epidermal cells. Wnt has been found to be an important switch in this process, followed by SHH protein downstream from this (Gentile and Garcovich, 2020).
The first plasma concentrates to be developed for use in surgery were platelet-rich plasma (PRP) in 1998 and plasma-rich growth factors (PRGF) in 1999, followed by platelet-rich fibrin (PRF) in 2001 (Dohan et al, 2006; Gianni et al, 2015; Gentile and Garcovich, 2020). Their first uses were for bone grafting for implants, tissue repair and wound healing within the field of maxillofacial dentistry. Experimental studies with concentrates began in the field of hair transplantation in 2006, and, by 2011, studies emerged using PRP for AGA alone (Dohan et al, 2006; Gianni et al, 2015; Gentile and Garcovich, 2020). The complete list of growth factors identified in PRP and their suggested biomolecular pathways in the treatment of AGA are detailed in Table 1.
Table 1. Growth factors identified in PRP and their suggested bio-molecular pathways
| Growth factors | Biomolecular pathway in hair regrowth |
|---|---|
| Vascular endothelial growth factor (VEGF) | Improves perifollicular angiogenesis; elevated expression in dermal papilla cells during anagen phase; endothelial cell-specific mitogen; microvascular permeability and perifollicular vascularisation |
| Epidermal growth factor (EGF) | Improves the activity and growth of follicle outer-root sheath cells by activation of Wnt/β-catenin signalling; cell growth modulator during follicular differentiation; proliferation and migration of follicular outer root sheath cells |
| Fibroblast growth factor (FGF) | Improves the advancement of hair follicles; anagen phase induction via β-catenin expression; angiogenesis; dermal fibroblast and hair follicle mitogen |
| Platelet-derived growth factor (PDGF) | Upregulate the genes associated with HF separation, induction and control of anagen; angiogenesis and vascularisation; hair follicle dermal stem proliferation; mesenchymal stem cell mitogen |
| Insulin-like growth factor 1 (IGF-1) | Improves the migration, survival and proliferation of HF cells; hair follicle proliferation during development; increase hair density and inhibit apoptosis |
| Hepatocyte growth factor (HGF) | Enhance the proliferation of follicular epithelial cells; hair follicle elongation; inhibits categan phase induction |
| Transforming growth factor beta (TGF-β) | Stimulates the signalling pathways that manage the hair cycle; extracellular matrix synthesis; fibroblast and mesenchymal stem cell proliferation; hair folliculogenesis and maturation |
| Interleukin 6 (IL-6) | Involved in WITN through STAT3 enactment |
| Insulin-like growth factor-binding protein 1 and 6 (IGFBP-1 to -6) | Manages the IGF-1 effect and its connection with extracellular matrix proteins at the hair follicle level |
| Bone morphogenetic proteins (BMP) | Maintains the DPC phenotype (fundamental for stimulation of HFSCs) |
| Bone morphogenetic protein type I (BMPR1) | Maintains the proper identity of the DPCs (basic for explicit DPC work) |
| Macrophage colony-stimulating factor (M-CSF) | Involved in wound-induced hair growth |
| Macrophage colony-stimulating factor receptor (M-CSFR) | Involved in wound-induced hair growth |
| Wnt3a | Involved in HF advancement through β-catenin signalling |
| Prostaglandin E2 (PGE2) | Stimulates anagen in HF |
| Prostaglandin F2 alpha (PGF2α) | Enhance change from telogen and anagen |
| 6-bromoindirubin-3'-oxime (BIO) | GSK-3 inhibitor |
| Prostaglandin D2 (PGD2) | Enhances follicle regeneration |
| Iron and L-lysine95 | Still under examination |
Injectable platelet-rich fibrin (iPRF) is an advanced liquid version of PRF and one of the latest blood products trialled for hair rejuvenation (Gianni et al, 2015). It is an autologous blood preparation containing stem cells and growth factors with high regenerative potential for hair rejuvenation (Arora and Shukla, 2019). iPRF is a relatively new concept and differs from conventional PRF preparations. iPRF is based on ideas that a lower speed of centrifugation yields maximum results with platelet, leukocyte and growth factor levels (Arora and Shukla, 2019).
The key properties of PRF are found in Table 2, while Table 3 highlights different strengths and weaknesses of PRP, PRGF and PRF.
Table 2. The key properties of Platelet-rich fibrin
| Purely autologous |
| No biochemical handling of blood |
| Cost-effective |
| Wound healing effects |
| Regenerative potential containing stem cells |
| Source of growth factors |
| Haemostatic effects |
| Supportive role in immune system |
| Sustained release of growth factors |
Table 3. Comparisons between autologous blood preparations
| Blood products | Platelet-rich fibrin | Platelet-rich growth factor | Platelet-rich plasma |
|---|---|---|---|
| Protocol | Easy | Complex | Very complex |
| Speed rate | Fast | Very slow | Slow |
| Reproducibility | No bias | Possible bias | Possible bias |
| Use of anticoagulants | No | Yes | Yes |
| Amount obtainable | Good | Poor | Enough |
| Costs of the protocol | Low | High | Moderate |
| Amount of fibrin obtainable | High | Low | Low |
| Speed of fibrin formation | Physiological | High | High |
| Fibrin morphology | Trimolecular | Tetramolecular | Tetramolecular |
| Leukocytes amount | 65% | 0% | 0-50% |
| Immunomodulatory properties | Yes | No | Poor |
| Neo-angiogenic potential | +++++ | ++ | + |
| Osteoconductive potential (scaffolding) | High | Poor | Poor |
| Mechanical properties (sol-gel-membrane) | Good | Poor | Enough |
| Presence of MSCs | Yes | Yes | Yes |
Methods and materials
The literature search strategy set out to answer three questions:
- Is there a preferred non-surgical autologous blood preparation to treat male AGA?
- Is there a non-surgical hair loss treatment preferred in combination with microneedling (MN) to treat male AGA?
- Is there a patient-reported outcome measure (PROM) preferred to evaluate non-surgical hair loss treatments relating to male AGA?
Searches began with sourcing English language titles using EMBASE and MEDLINE. The Cochrane Library Database and Centre for Controlled Registered Trials were also sourced. Supplementary searches involved scanning the reference lists of any relevant articles, which were then searched for in Pub.Med.gov. By following the trail of similar articles that were highlighted by the engine, extra sources were discovered and, where possible, accessed fully. All terms (medical subject headings (MeSH) or otherwise) were generally searched in relation to key words (‘ALOPECIA’, ‘ANDROGENIC ALOPECIA’, ‘PRF’, ‘PRP’, ‘PDGF’, ‘MICRONEEDLING’, ‘PATIENT-REPORTED OUTCOMES’, ‘COSMETIC DERMATOLOGY’ AND ‘PLASTIC SURGERY’), as well as the terms ‘SYSTEMATIC REVIEWS’ or ‘META-ANALYSIS’. Where such evidence was lacking, randomised controlled trials (RCTs), controlled clinical trials or clinical trials were included. Pilot studies, case studies and in-vitro and animal studies were included where deemed highly relevant. Female AGA studies were excluded initially, as were letters to editors, expert opinions and non-English articles. Included articles were retrieved in full. Data extraction followed pre-defined criteria and included both study-specific issues, such as a study design, respondent characteristics and instrument-specific issues.
Results and discussion
Despite the widespread use of PRP, concerns have been raised about its two-step process requiring the use of thrombin and anticoagulants. These can impair wound healing by inhibiting the coagulation process (Dohan et al, 2006). In response to this, PRF was developed as a second-generation platelet concentrate in 2001 (Dohan et al, 2006; Arora and Shukla, 2019). Obtained using a one-step centrifugation process without the use of anticoagulants, it is completely autologous. The resulting fibrin matrix contains platelets, leukocytes and mesenchymal stem cells. PRP lacks regenerative potential, as compared to PRF (Arora and Shukla, 2019). Depending on the blood collection tube and centrifugation protocol used, solid gel and liquid forms of PRF can be developed (Schiavone et al, 2018; Arora and Shukla, 2019).
Further complexities exist due to variations in kinds of PRP and PRF, depending on their cell content and fibrin architecture, see Table 4 for further detail.
Table 4. Platelet-rich plasma and platelet-rich fibrin cell content and fibrin architecture
| Type | Description |
|---|---|
| Leukocyte-poor platelet-rich plasma (LP-PRP) or pure PRP (P-PRP) | PRP without leukocytes and with a low-density fibrin network after activation |
| Leukocyte-PRP (L-PRP) | PRP with leukocytes and a low density fibrin network after activation (most frequent) |
| Leukocyte-poor platelet-rich fibrin (LP-PRF) or pure PRF (P-PRF) | PRF without leukocytes and a high-density fibrin network |
| Leukocytes PRF (L-PRF) | PRF with leukocytes and a high-density fibrin network |
PRP tends to yield approximately 300-700% enrichment of platelets. However, the optimum concentration remains unclear. Heterogeneity between studies and lack of standardisation in methods can be reduced using the FIT PAAW tool, which is detailed in Table 5. While consensus is lacking, the challenge to find direct comparisons and reliable statistical analysis remains.
Table 5. FIT PAAW classification
| Acronym | Description |
|---|---|
| F | Force of centrifugation |
| I | Iteration or sequence of centrifugation |
| T | Time of centrifugation |
| P | Platelet concentration |
| A | Anticoagulant use |
| A | Activator (type and amount) |
| W | White blood cell count |
MN has arisen as a beneficial therapeutic option for hair rejuvenation within clinical and aesthetic dermatology over the past two decades (Iriarte et al, 2017; Ramaut et al, 2018). Yoon et al (2016) studied hair growth in murine species. After repeated microneedle stimulation five times a week for 3 weeks, the study proved that, even alone, MN can stimulate stem cells in the dermal papillae, increase blood flow to hair follicles and enlist growth factors and signalling pathways to bring about hair restoration (Yoon et al, 2016). They prophesied that MN could lead to new breakthroughs in treating alopecia, especially when combined with the drug delivery effect. This effect is possible because the microinjuries (holes) or micro-conduits created allow for adjuvant enhancement in the topical absorption of prescription, cosmeceutical or cosmetic products across the thick stratum corneum (Yoon et al, 2016).
Two systematic reviews linking MN to AGA represent the only in-depth evidence available (Ramaut et al, 2018; Zhou et al, 2020). Ramaut et al's (2018) systematic review includes two studies that meet inclusion criteria. First, Dhurat et al's (2013) prospective, evaluator-blinded RCT, resulting in statistically significant improvement in mean hair counts following the use of MN (using a roller device with a 1.5 mm needle depth) and minoxidil over 5% minoxidil alone (Dhurat et al, 2013). Second, Dhurat and Mathapati's (2015) study explored the adjunct benefits of MN for 6 months, alongside daily finasteride and 5% minoxidil use. Subjects were followed up 18 months post treatment to measure sustainability of response. All showed two or three grade improvements using a seven-point standardised evaluation scale and subjective hair growth assessment scales. No adverse effects were reported (Dhurat and Mathapati, 2015).
Zhou et al's (2020) systematic review also includes a meta-analysis (Zhou et al, 2020). They highlighted three further studies. When searched, these studies all appeared in the list of Cochrane Library published trials. Four of the 15 studies comprised a cluster of combined MN and minoxidil versus minoxidil alone trials. After removing one that caused main heterogeneity (Yu et al, 2018), the other three studies (192 patients) underwent the fixed effect model used in meta-analysis with the absence of heterogeneity (l2 = 0%), proving that combination therapy was superior to monotherapy. Studies were also measured in terms of global photographic assessment (p<0.05) and showed a significant increase in hair count (95% confidence interval, 1.32-1.98; p<0.05) compared to monotherapy. Quality assessment and data analysis were performed by Review Manager 5.3 (Kumar et al, 2018; Bao et al, 2020).
Overall, Ramaut et al (2018) and Zhou et al (2020) both conclude that treatment combinations using MN are safe and effective for scars and wrinkles, but that further research and improved methodological study design are needed to echo this for AGA (i.e. multi-centre RCTs with use of histology). Zhou et al (2020) concluded that combination therapies do report greater efficacy than monotherapies, and combination therapies are preferable over monotherapy. Once again, they state that further RCTs are needed to prove this. Adverse events were rare when MN was combined with minoxidil and side effects were minimal (Zhou et al, 2020). Other studies combining the use of PRP with MN and minoxidil have been undertaken successfully but were not included in these systematic reviews (Farid and Abdelmaksoud, 2016; Shah and Shah, 2017; Jha et al, 2019).
While over a dozen systematic reviews exist using PRF in dentistry and plastic and reconstructive surgery, evidence is lacking within the field of non-surgical hair rejuvenation. Through the literature searches, two trials were found to employ a MN device to deliver the PRF in combination with mesotherapy injections (Schiavone et al, 2018; Arora and Shukla, 2019). Table 6 details some of these key findings. While 75% of inclusive studies were controlled, they lacked randomisation, blinding and large numbers. Scalfani (2014) used a hair density index to measure hair density and thickness. All studies showed higher patient satisfaction in low grade AGA (Scalfani, 2014). Once again, comparisons are hindered through varying protocols for preparing blood concentrates and lack of standardisation. Further in-depth RCTs are needed.
Table 6. Results of literature review on platelet-rich fibrin and microneedling
| Author, date | Study type, level of evidence | Key outcomes | Study weakness |
|---|---|---|---|
| Nanditha et al, 2017 | Systematic review and meta analysisLevel IA | Included systematic reviews, randomised controlled trials and pilot and case studies searched from MEDLINE, Google Scholar and Science Direct from 2008-July 2017 | Did not categorise the study designs while evaluating success ratesRecognises that further long-term studies are needed in distinct areas to decisively prove effectiveness Only covers Scalfani study (see below) |
| Picard et al, 2017 | Systematic reviewLevel IA | Only used studies clinically assessing the efficacy of platelet-rich plasma (PRP). Searched up to February 2017 in PubMed and Google Scholar. It included 14 articles | Only covers Scalfani study Used PRP as an umbrella term for platelet-rich fibrin (PRF) |
| Scalfani, 2014 | ProspectiveCohort studyLevel IINine males, 6 females with long-term mild to moderate AGA. Aged under 40 yearsDid not use microneedling | Three-times treatment on monthly basis with PRF matrix. Hair density index (HDI) outcome measured at 1,2, 3 and 6 months post treatment. Subjects with 25% improvement by 1 month likely to have same at 6 months post treatment | Uncontrolled, no histologyLow numbersNeed longer follow-upWide variability of responsesOnly worked in mild casesHDI decreased to 75.1% 4 months after last injectionNo correlation found betweenNorwood classification and age to prove results |
| Mahapatra et al, 2016 | Controlled studyLevel III10 males, grade 4-6 on the Norwood scale. Study to evaluate iPRF as adjunct to FUE. Three intradermal injections given.First prior to FUE then at 2 and 3 months. Follow-up at 6 months. | Statistical analyses were made with the student's t-test. A value of P<0.05 indicated statistical significance. Observed a statistically significant difference before and after implantation when compared to controlNo microneedling used | Further and longitudinal studies needed to understand and evaluate regenerative and retention properties of PRFMCompare PRFM with FUE, not PRFM aloneNo histology |
| Schiavone et al, 2018 | Controlled prospective studyLevel III168 patients recruited. Each were given two treatments, 3 months apart. Treatment group and control group. Baseline and 6-month macrophotographs were taken. They were rated by a 5-person expert panel (blinded), using the 15-point Jaeschke scale to evaluate clinical change | Overall differences in clinical change between treatment and control group always reached statistical significance for each observer (p <.001). The more severe the AGA, the greater the clinical difference measured.Microneedling using 1-2mm dermapen | ACD-A anticoagulant added Patients taking MX or Finasteride for 1 year remained on drug thoughout trialNeed longer term follow-upNot randomisedNo histology |
| Arora and Shukla, 2019 | Case reportLevel IVThree cases of male AGA (type I, VI and VII). Four treatments of iPRF every 15 days (Cleopatra technique), delivered in combination with microneedling using Dermapen | All cases reported pain free experience with mild bruising and inflammation. Measured by clinical outcomes and subjective questionnaire based on patient satisfaction. Type I and VI satisfied with hair growth after 4 treatments. Slight growth in type VII, and so took more treatments. | No control groupsNeed larger sample size and longer duration of follow-upSuggest extending to 6-7 sessionsNo histology |
Evidence does show that the combination of PRF and MN is safe and effective, with ongoing treatment recommended (for example, one per month for 3 months and then one treatment every 3 months) for optimum results (Schiavone et al, 2018). Again, there are few contraindications, as with PRP. Mild to moderate pain and limited side effects were reported generally. The largest trial, which was conducted by Schiovone et al (2018), is a promising advert for iPRF and MN combined. Only 15% of patients in this study experienced transient bruising for 48-72 hours post treatment, which spontaneously healed after 4-5 days. Schiovone et al's (2018) protocol yielded a five-fold increase in fibrinogen values, roughly a 4.5-fold increase in platelets concentration and lymphocyte numbers and nearly a two-fold increase in granulocyte numbers (Schiovone et al, 2018).
Nevertheless, the most recent systematic review by Gentile et al (2020) reveals that PRP publications are on the rise compared to PRF. Between 2015-2019, a total of 137 articles focused on the use of PRP in AGA were published, compared to 18 between 2011-2014. Gentile et al (2020) stated that the future vision for PRP is to overtake the use of minoxidil, finasteride and dutasteride, and, as authors, advocated the case. They called for further low risk of bias RCTs and standardised protocols to be trialled through larger multicentre trials, to establish reliable and reproducible results among clinicians (Gentile et al, 2020).
The advantages of PRP are the low side effect profile, lower cost (in theory—further studies are needed) and effectiveness for males with low-to-moderate AGA. There are few contraindications; autoimmune disease, thyroid disorders, bleeding disorders or other coexisting morbidities are the main ones. However, if treatment is stopped, unfortunately, hair does fall out (Evans et al, 2020; Gentile et al, 2020). Studies recommend performing at least three injections 1 month apart, followed by regular maintenance treatments every 1-3 months. Ideally, for consistency, treatment should be delivered through mechanical and controlled injections. Combination options are growing for PRP, and practitioners need to keep up with this trend. Needless to say, combination treatments will compound further debate around protocols and standardisation comparisons (Lotti et al, 2019; Evans et al, 2020; Gentile et al, 2020; Hesseler and Shyam, 2020).
Conclusion
In adulthood, epithelia and blood-forming tissues remain highly mitotic, which provides a constant reserve for use in regenerative aesthetic medicine (Richards and Merharg, 1995). Quantitatively, evidence still exists to suggest that, at present, PRP is the preferred blood preparation for treating male AGA (Evans et al, 2020; Gentile et al, 2020). However, studies exist to prove that, in theory, iPRF has greater regenerative potential than PRP (Arora and Shukla, 2019).
Research also suggests that MN, in combination with minoxidil therapy, is preferred over iPRF and MN at present. One study has proven that PRP treatment with MN is better in comparison with PRP alone or minoxidil monotherapy in patients with male AGA (Kumar et al, 2018). Additionally, studies show that iPRF combined with MN is a safe and effective option for the treatment of male AGA. However, comparison studies against other combinations are lacking (Schiavone et al, 2018; Arora and Shukla, 2019). Unless a specific PROM is developed and validated for male AGA, challenges around treatment comparison will continue to limit evidence.
Key points
- Studies have emerged to prove that platelet-rich fibrin (PRF) has greater regenerative potential than platelet-rich plasma (PRP) prepared with additives
- Quantitatively and, to some degree, qualitatively, evidence exists to suggest that PRP is the preferred blood preparation for treating male androgenetic alopecia (AGA), in combination with microneedling and minoxidil therapy
- Nevertheless, studies show that iPRF combined with microneedling is a safe and effective option for the treatment of male AGA, but comparison studies against other combinations are lacking. Further low-risk of bias randomised controlled trials and standardised protocols need to be studied through larger multicentre trials to establish reliable and reproducible results
- No validated patient-reported outcome measures (PROMs) currently exist for male AGA. Unless a specific PROM is developed and validated for male AGA, challenges around treatment comparison will continue to limit evidence.
CPD reflective questions
- In theory, why is platelet-rich fibrin (PRF) thought to be more effective than some preparations of platelet-rich plasma (PRP)?
- Which growth factor is most linked to hair follicle stimulation?
- Which other treatments can be combined with PRP/PRF to treat hair loss?