


There is growing evidence supporting the use of a holistic approach in dermatology for patient treatment so as to increase the success rate and relapse prevention. Combining these alternative approaches, along with traditional medical treatments, yields better, long-term outcomes (Hughes, 1983; Carey Cole, 1988; Ehlers et al, 1995; Kabat-Zinn et al, 1998).
Approximately 17% of dermatology patients need psychological support and 14% have a psychological condition exacerbating their skin disease (Bewley et al, 2012). Research also provides a strong link between lifestyle factors and inflammation at skin level, (Naldi et al, 1999; Cordain et al, 2002; Li et al, 2017). Nurses who take time to explore triggers, provide education and involve patients in the prescribing process will achieve better treatment outcomes for their patients (Courtenay et al, 2009).
The author finds it useful to explore psychological and lifestyle factors with all new clients using a ‘five pillars’ consultation process, encouraging them to speak openly about different areas of their lives from the start of their treatment programme.
Psychodermatology
Psychodermatology addresses interactions between the mind and the skin (Jafferanay, 2011), and has recently seen a rise in popularity in UK dermatology clinics, possibly due to a recent study that showed that 86% of dermatology subjects who received psychological input at the Royal London Hospital were discharged after just one follow-up appointment (Shah et al, 2015). The link between the emotional state of the patient and skin disease is well-documented, with numerous human and murine studies providing evidence that the skin has its own hypothalamic-pituitary axis, perpetuating stress responses where cortisol levels are raised even for short bursts of time, causing skin barrier compromise, reduced epidermal hydration and thickness and disruption of mitochondrial DNA repair and production, (Misery, 1996; Aioi et al, 2001; Jaffaranay, 2007; Romana-Souza et al, 2011, Allen et al, 2018; Singh et al, 2018).
Furthermore, many studies have provided evidence of significant skin disease symptom improvement when stress-reducing therapies are implemented in combination or alongside orthodox medicine; combining biofeedback-assisted relaxation therapy with cognitive therapy reduced acne severity in 30 patients, (Hughes, 1983). Combining psoralen ultraviolet light A (PUVA) or type B ultraviolet (UVB) light therapy with audio-mindfulness accelerates psoriatic lesion clearance in patients with moderate to severe disease, even in short bursts (Kabat-Zinn et al, 1998). Up to 93% of alopecia araeta patients will experience depression (Abarbi et al, 2013), and one study provided evidence that six sessions of hypnotherapy accelerated hair regrowth in 57% of alopecia araeta patients (n=21), which continued after hypnosis cessation, (Willemson et al, 2006). Symptom improvement and reduced topical agent use was seen in atopic dermatitis patients treated with combination therapies including group, cognitive behavioural and autogenic (Cole et al, 1988, Ehlers et al, 1995).
It is important also to realise that skin conditions themselves can cause anxiety, sadness, feelings of embarrassment and humiliation in an individual, irrespective of its severity or type (Shah 2012), and there is evidence of increased suicidal ideation in patients with psoriasis (7.2%) and acne vulgaris (5.6%), compared to the general population (Gupta et al, 2003).
 Acne vulgaris, along with various other skin conditions, can cause low self-esteem, anxiety and embarrassment in patients
Acne vulgaris, along with various other skin conditions, can cause low self-esteem, anxiety and embarrassment in patients
Although evidence suggests social media interaction reduces feelings of isolation and anxiety, boosting self-esteem and overall wellbeing (Wang et al, 2014), many societies around the world perceive that skin that is unblemished is tantamount to beauty, and even success. Many of the images we face through social media channels exhibit perfection, which may induce feelings of inadequacy (Shah, 2012).
Psychodermatology provision nationally declined between 2003 and 2011 (Bewley et al, 2012). As a result, the British Association of Dermatologists provided guidelines for setting up psychodermatology branches in clinics in 2012, emphasising the importance of allowing adequate time during initial assessment for assessing psychological status of each individual patient, and using psychometric tools such as Annual DLQI and Skindex 29 for all those with long-term and/or disfiguring skin conditions (Bewley et al, 2012). The guidelines also suggest accessing referral networks in the local community and undertaking appropriate staff training. Stepped provision of psychodermatology services can also be referred to in Figure 1 (Bewley et al, 2012). Undertaking this process may seem like a challenge for busy practitioners, but the long-term implications for better treatment outcomes and time-saving is evident (Shah et al, 2015).
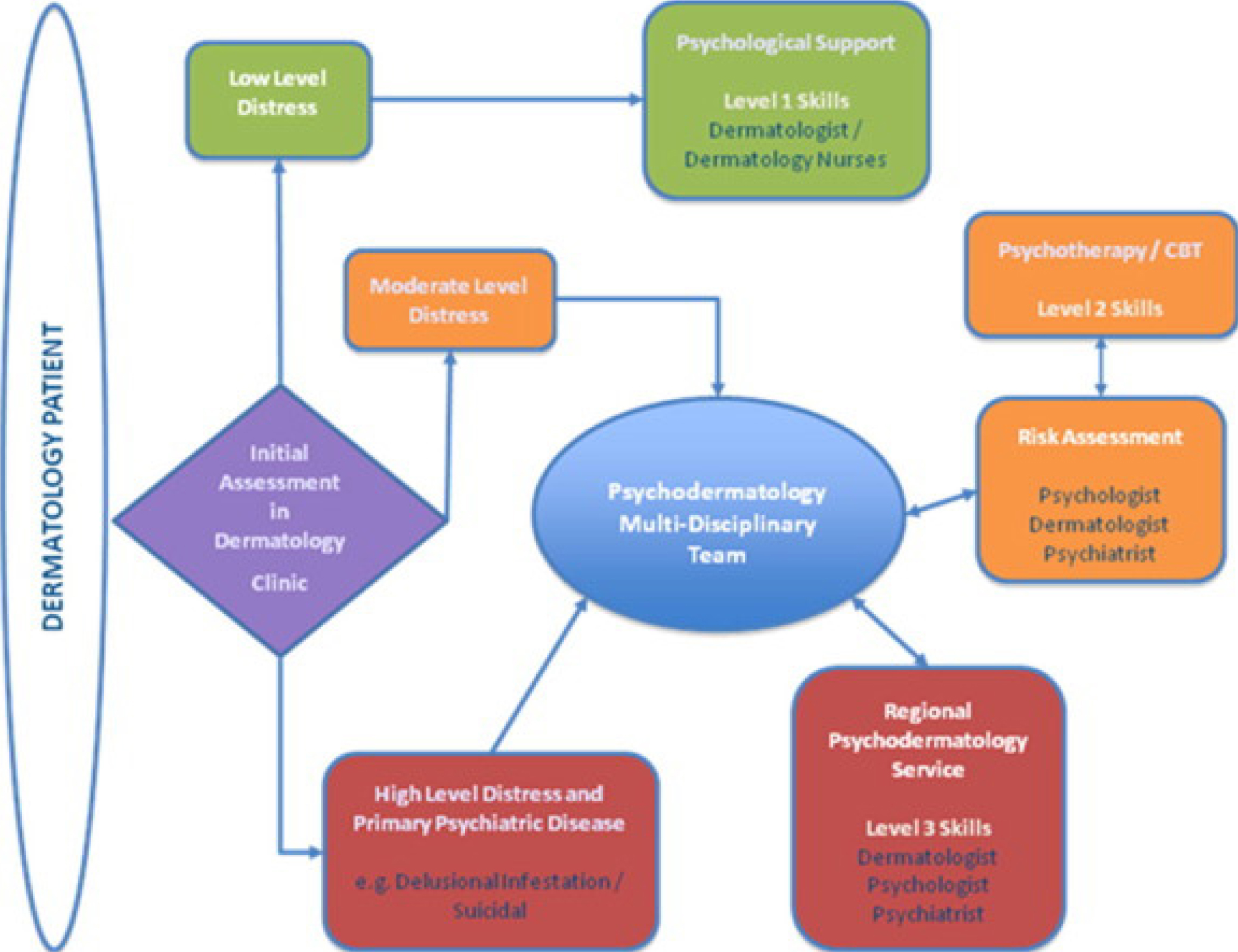 Figure 1. Stepped provision of psychodermatology services
Figure 1. Stepped provision of psychodermatology services
Lifestyle factors
Stress
Certain lifestyle choices that place the body and mind under stress are known to disrupt skin barrier function and cause inflammation. Over a third of people in the UK experience stress for up to 9 days each month, and the most common triggers are work, finance and health concerns (forthwithlife.co.uk, 2018, mentalhealth.org.uk, 2018). To prevent and control inflammatory flare ups, the author makes plans for clients, including realistic and attainable choices to counteract stressors in their lives. One example is implementing yoga, or at least regular episodes of yoga breathing, as there is evidence to suggest that 10–30 minutes of daily pranayama (yogic breathing exercises) significantly reduces free radicals, systolic and diastolic blood pressure and existing stress levels, as well as reactions to further stressful stimuli (Bhattacharya et al, 2002; Telles S et al, 2013). Fresh air and moderate exercise such as walking in a rural location can also significantly improve feelings of wellbeing (Roe et al, 2011).
Alcohol
There is much evidence supporting prolific incidence of alcholism in psoriatic patients and increased risk of pustular lesions (Brenaut et al, 2013), with up to 30% of sufferers identified as having difficulties with alcohol (Kirby et al, 2008).
One large scale US study showed that women with a history of consuming seven or more alcoholic drinks weekly—particularly white wine and spirits—displayed an increased risk of melanoma and non-melanoma skin cancer development (Kubo et al, 2014). Another large scale study conducted over 14 years with female rosacea patients showed a significant increase in flare-up risk, particularly in those who regularly consumed white wine and spirits (Li et al, 2017). While there is a link between alcohol consumption and raised IgE levels, there is no current evidence supporting significant links with atopic dermatitis (Berglind et al. 2011; Lomholt et al, 2016). There is also some data showing that 15% of vitiligo sufferers are addicted to alcohol, likely to lead to poor treatment compliance and significant increase in disease duration and severity (Zaghloul et al, 1991; Yaswanth et al, 2015).
Diet
Although controversial, some studies highlight a link between psoriasis, insulin resistance and obesity (Boehncke et al, 2007). One study provided evidence that a low calorie diet administered to patients with non-pustular psoriatic lesions improved skin lesions, although only 38% of subjects experienced significant weight loss (Rucevic et al, 2003). Another Italian study highlighted significant links between consumption of carrots, tomatoes and fresh fruit with psoriatic lesion clearance (Naldi et al, 1996).
Acne vulgaris is viewed as a disease of western culture, affecting 79–95% of adolescents and 40–54% of men and women aged over 25 years in these societies, yet, it is practically non-existent amongst Asian populations. This is thought to be attributed not only to genetic factors, but also diet (Cordain et al, 2002). There is evidence that daily consumption of two glasses of full fat or skimmed milk significantly increases acne risk, while a low BMI and eating fish three times weekly appears to exert a protective effect (Landro et al. 2012). Another Turkish paper describes a positive correlation between high glycaemic index diet and acne development in 50 subjects (Çerman A et al, 2016). In regard to skin cancers, an Australian study highlighted a link between frequent fish consumption, pulses, green and dark coloured vegetables and lowered nonmelanocytic cancer risk (Kune et al, 1992).
» The protective, moisturising and anti-inflammatory benefits of flavonoids, curcuminoids, niacinamides and peptides found in polyphenols are being increasingly explored and documented as helping to combat effects of environmental and emotional stressors «
‘Milkshake’ diets have grown in popularity amongst several of the author's patient groups looking for accelerated weight loss in preparation for an upcoming event or new relationship. Links between hair loss and diet have been well documented, believed to be due to iron and zinc deficiency causing a reduction in hair follicle and hair matrix energy supply (Follis et al, 1941; Detlef et al, 1976).
Smoking and e-cigarettes
Today, more than 10% of US, European and Asian populations use e-cigarettes (Bousquet et al, 2015). Early murine studies suggest that vaping disrupts skin healing in the same way that cigarette smoking does, due to additives such as propylene glycol, which can trigger allergic immune responses similar to eczema, rhinitis and asthma in users (Bousquet et al, 2016; Troiano et al, 2019). Long-term dermatological effects of e-cigarette use remains unknown at present.
Traditional smoking doubles the risk of squamous cell carcinoma development, thought to be due to mutation of p53 gene expression (Brennan et al, 1995; Simpkin et al, 2016). In psoriasis, there is a strong association between pustular lesion formation and female smokers (Naldi et al, 1999) and discoid lupus erythematous lesion risk increases tenfold with smokers (Simpkin et al, 2016). One national study provided evidence of significant links between hand eczema and smoking, confounded by presence of allergic medical history (Berglind et al, 2011). Smoking contributes to hair loss in many ways: through disruption of dermal hair papilla microcirculation, follicular inflammation and fibrosis, hair follicle DNA damage and lowered estradiol levels, caused by increased hydroxylation (Trueb, 2003).
Sleep
Patients with pruritic skin conditions often experience worsening of the itch at night, causing sleep disruption and thought to be due to natural cortisol trough at this time of the day (Gupta et al, 2013). Approximately 94% of patients with chronic dermatology conditions report sleep problems, thought to be due to substance P stimulation, which effects mood and skin inflammation, but further research is needed (Anderson et al, 2006). Correlations between chronic skin disorders, mood and sleep have been documented, with issues such as anxiety and depression likely to worsen sleep quality (Mostaghimi, 2008).
Probiotics
Seventy years ago, two dermotologists, John Stokes and Donald Pillsbury, hypothesised that the emotional state of a person (depression, worry and anxiety) will affect gut micro flora by causing small intestine bacteria overgrowth (SIBO), contributing to skin inflammation, particularly in cases of acne vulgaris, atopic dermatitis and rosacea (Parodi et al. 2008; Guencihe et al. 2010; Chang et al, 2016). Findings from one study suggest that lactobacillus paracasei therapy inhibits substance P-induced inflammation (Guencihe et al, 2010), while a combination of pre- and probiotics is recommended for symptom control in atopic dermatitis patients (Chang et al, 2016). Although more work is required in this area, the author regularly prescribes probiotics for the aforementioned patient groups, and many positive outcomes have been witnessed when combined with other treatments.
Skincare and cosmetics
There is evidence to suggest that certain skin cleansers and soaps with a pH of 8.0, and certain hair pomade products are comedogenic and likely to cause or worsen acne eruptions (Plewig et al, 1970; Tarun et al, 2014).
 Probiotics can have positive outcomes for patients when combined with other treatments
Probiotics can have positive outcomes for patients when combined with other treatments
The protective, moisturising and anti-inflammatory benefits of flavonoids, curcuminoids, niacinamides and peptides found in polyphenols are being increasingly explored and documented as helping to combat effects of environmental and emotional stressors (Bogdan Allemann et al, 2008).
Topical lipids such as ceramides alongside emollients help to restore stratum corneum homeostasis and skin barrier function (Draelos, 2018).
Conclusion
Many studies quoted are small scale and further global, long-term research is required to pinpoint exact mechanisms of how balancing mind and body leads to better skin health. Further studies on how gene P53 and substance P functions are affected by psychosocial and lifestyle would also be beneficial in helping us to gain a better understanding of causes and treatments. Development of psychodermatology clinical governance protocols by the British Association of Dermatologists would facilitate private clinicians in implementing a psychodermatology branch (Bewley et al, 2012).
Key points
- The British Association of Dermatologists has recognised a need for incorporating psychodermatology into skin disease management plans in leading to better treatment outcomes
- A recent UK study found that 86% of dermatology out-patients who received integrated treatment were discharged after one follow-up, saving time and money for the department
- There is increasingly emerging evidence to support the impact that lifestyle can have on skin disease and how educating patients about this aspect may prevent relapse
- Gaining a better understanding of how gene P53 and substance P functions are affected by psychosocial and lifestyle factors may give dermatology practitioners insight into how best to treat patients
CPD reflective questions
- What proportion of the dermatology patients in your practice setting would you say, show signs of stress and anxiety as a direct result of their skin problem?
- What protocols do you have in place for your patients with chronic, life changing skin diseases and high quality of life (DLQI or similar), scores?
- How can dermatology nurses and practitioners support patients in making relevant lifestyle changes?